A laboratory result is only as reliable as the specimen it was derived from. Before a single analytical measurement is made, the sample traveling from a patient’s vein to a clinical laboratory has passed through a chain of collection, labeling, packaging, transport, and receipt steps, each of which carries its own opportunity for error. When those errors compromise specimen integrity to the point where analysis would produce misleading or dangerous results, the laboratory has both a professional and regulatory obligation to reject the sample. This process, governed by documented specimen rejection criteria, sits at the intersection of patient safety and diagnostic accuracy.
Understanding specimen rejection criteria in clinical laboratories is not just a technical concern for laboratory professionals. It affects every nurse drawing blood on a busy inpatient unit, every phlebotomist working through a high-volume outpatient draw station, every clinician waiting on a coagulation result before starting anticoagulation therapy, and every patient who must undergo the discomfort and delay of a repeat collection. When rejection rates are high, turnaround times lengthen, costs rise, and the risk of incorrect clinical decisions increases. When rejection criteria are poorly defined or inconsistently applied, laboratories produce results from compromised specimens, creating a different but equally serious patient safety problem.
This article examines what specimen rejection criteria are, which causes of rejection appear most frequently in the published data, how rejection rates vary across collection settings and test types, what the downstream consequences of rejection are, and what practical strategies have been shown to reduce rejection rates without compromising analytical quality.
What Specimen Rejection Criteria Are and Why They Exist
Specimen rejection criteria are the documented, pre-established conditions under which a clinical laboratory will decline to analyze a submitted sample and request a new one. These criteria are required under multiple regulatory and accreditation frameworks. ISO 15189, the international standard for medical laboratory quality and competence, specifically requires that laboratories develop documented procedures for acceptance and rejection of specimens. The Clinical Laboratory Improvement Amendments (CLIA) in the United States impose parallel requirements, and accrediting bodies such as the College of American Pathologists (CAP) and The Joint Commission expect laboratories to maintain written rejection policies with supporting rationale.
The underlying logic is straightforward. Certain specimen conditions, whether caused by collection technique, transport handling, or patient physiology, introduce interferences or analyte changes significant enough to make results clinically unreliable. Reporting those results would be worse than reporting nothing at all, because a clinician acting on a falsely elevated potassium or a spuriously prolonged prothrombin time may cause direct harm. Rejection criteria define the threshold at which the risk of a wrong result outweighs the inconvenience and delay of recollection.
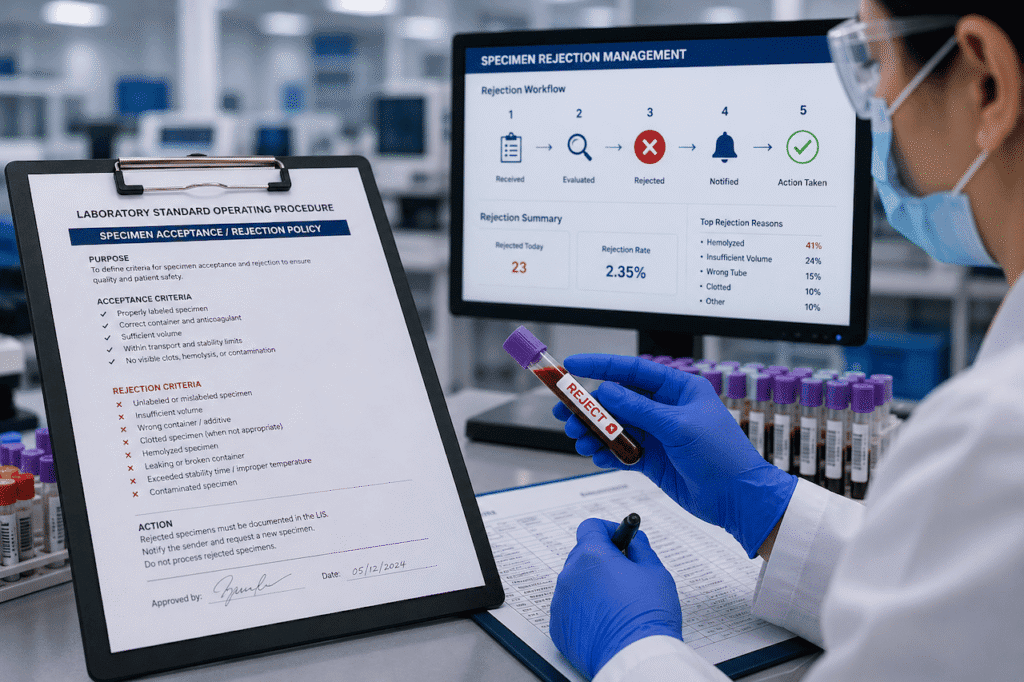
Rejection criteria are divided into two general categories. Universal or absolute rejection criteria apply regardless of the test being requested. These include specimens with no patient identification or mismatched identification between the tube and the accompanying order, specimens with no label at all, samples received in leaking or broken containers, and specimens collected in containers that are incompatible with the requested test at a fundamental level, such as a coagulation test submitted in an EDTA tube. Conditional or test-specific rejection criteria apply only to particular analytes or disciplines. Hemolysis may be an absolute rejection criterion for potassium but only a conditional one for albumin. A frozen sample that thawed in transit is unacceptable for coagulation studies but may still be analyzable for certain immunoassays depending on the analyte’s stability profile.
The Data on How Often Rejection Happens and Why
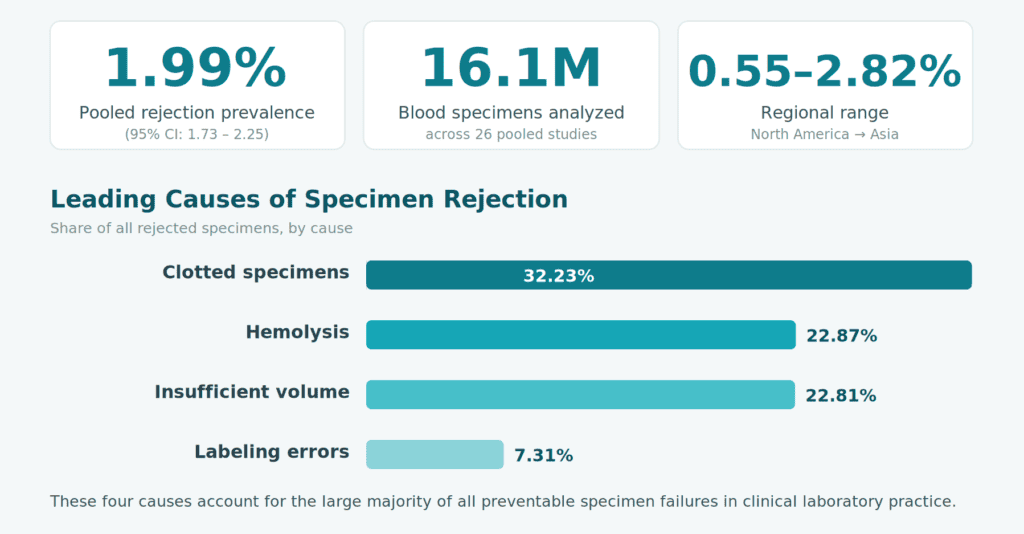
A 2022 systematic review and meta-analysis published in a peer-reviewed journal, drawing on data from 16,118,499 blood specimens across 26 studies, established the pooled prevalence of blood specimen rejection in clinical laboratories at 1.99 percent (95% CI: 1.73 to 2.25). The range across regions was substantial: rejection prevalence was highest in Asia at 2.82 percent and lowest in North America at 0.55 percent. Quality programs tracked by the College of American Pathologists have reported aggregated rejection rates ranging from 0.30 percent in outpatient facilities to 0.83 percent in hospital-based laboratories, though individual institutions operating in high-acuity environments often exceed these figures considerably.
The leading causes identified across that meta-analysis were consistent with findings from individual institutional studies. Clotted specimens accounted for 32.23 percent of all rejections (95% CI: 21.02 to 43.43), hemolysis for 22.87 percent (95% CI: 16.72 to 29.02), insufficient volume for 22.81 percent (95% CI: 16.75 to 28.87), and labeling errors for 7.31 percent (95% CI: 6.12 to 8.58). Together, these four causes represent the overwhelming majority of preventable specimen failures in clinical laboratory practice.
What that pooled data does not fully convey is how sharply rejection rates vary by collection location and test type. A study conducted at Hacettepe University Hospitals across 453,171 samples received in a single emergency laboratory over 12 months found an overall rejection rate of 6 percent. Within that laboratory, rejection was concentrated in specific test categories: 13.3 percent of coagulation specimens, 12.8 percent of therapeutic drug monitoring samples, 12 percent of hormone tests, and 9.8 percent of blood gas specimens were rejected, compared to 2.5 percent for routine biochemistry tests. The ratio of rejected specimens was 40 percent higher in the emergency department than in intensive care units, and more than 40 percent higher than in inpatient services. A separate analysis published in the Archives of Pathology and Laboratory Medicine found that rejection rates in inpatient services were more than five times higher than in outpatient services, where trained phlebotomists rather than generalist clinical staff typically perform collections.
These patterns reflect a core reality of specimen rejection: most rejections are not a laboratory problem. They are a clinical problem that the laboratory detects.
Clotted Specimens: The Single Largest Cause of Rejection
Clotting accounts for the largest individual share of specimen rejections worldwide, and the reasons are well understood. Blood collected for hematology or coagulation studies must be properly mixed with an anticoagulant immediately after collection, typically by inverting the tube four to eight times depending on the tube type. When that mixing does not occur promptly or adequately, the coagulation cascade activates within the tube, forming fibrin clots that interfere with automated analyzers and invalidate results entirely for coagulation studies. In oncology settings, a study published in ScienceDirect found that clotted specimens accounted for 43.8 percent of all rejections, and a similar institutional study reported clotting as the most common rejection reason at 51.2 percent. Inappropriate mixing of blood with the anticoagulant after collection was identified as the primary explanation.
The coagulation laboratory is particularly vulnerable to clotting-related rejections because citrate tubes used for prothrombin time and activated partial thromboplastin time testing require a precise 9:1 blood-to-anticoagulant ratio. An underfilled tube dilutes the anticoagulant, while an overfilled tube reduces it, both of which invalidate the coagulation result. The Clinical and Laboratory Standards Institute specifies that specimens must be filled within 10 percent of the manufacturer-stated draw volume to achieve the correct ratio. According to a study published in ScienceDirect, tubes filled below 30 percent of their intended volume are significantly more prone to both clotting and hemolysis.
Hemolysis: The Most Clinically Consequential Rejection Reason
Hemolysis, the rupture of red blood cells with release of intracellular contents into the surrounding plasma, is the most complex of the major rejection causes because it is simultaneously a collection artifact, a potential pathological finding, and an analytical interference that varies dramatically by analyte.
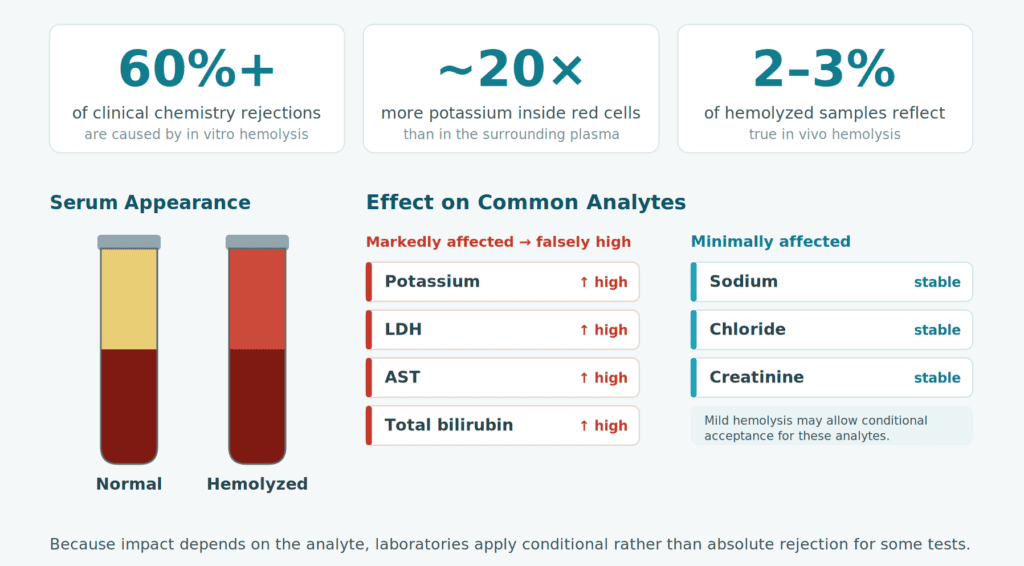
In vitro hemolysis, caused by phlebotomy technique errors or improper handling rather than a patient’s disease, accounts for over 60 percent of clinical chemistry sample rejections worldwide according to a 2026 analysis published in the Journal of Analytical Methods in Chemistry. Causes include drawing blood through a small-gauge needle at high vacuum, using butterfly needles without adequate filling before tube transfer, shaking rather than gently inverting tubes, exposure of samples to temperature extremes during transport, and prolonged delays between collection and processing. In the emergency department specifically, hemolysis rates have been documented as high as 25 to 30 percent of submitted specimens, with specimen rejection rates exceeding 4 percent, significantly above hospital-wide averages. This reflects the realities of emergency phlebotomy: urgent collection under suboptimal conditions, frequent use of peripheral IV lines as draw sites, and limited time for technique refinement.
The clinical consequences of hemolysis depend entirely on what is being measured. Potassium is among the most dramatically affected analytes because erythrocytes contain a concentration of potassium approximately 20 times higher than plasma. A hemolyzed specimen can produce a falsely elevated potassium reading that triggers clinical intervention for a hyperkalemia that does not exist, including modification or cessation of cardiac medications in a patient whose true potassium is entirely normal. Lactate dehydrogenase, aspartate aminotransferase, and total bilirubin are similarly affected. In contrast, analytes such as sodium, chloride, and creatinine show far less interference from hemolysis, which is why conditional rejection criteria rather than absolute rejection are appropriate for some tests in the presence of mild hemolysis.
The distinction between in vitro and in vivo hemolysis is also clinically meaningful. Only 2 to 3 percent of all hemolyzed samples contain hemolysis from an underlying patient condition such as autoimmune hemolytic anemia or disseminated intravascular coagulation. When in vivo hemolysis is suspected, rejecting the sample is not appropriate, because the patient’s condition genuinely causes elevated intracellular analyte concentrations that are diagnostically relevant. Laboratories managing hemolyzed specimens from critically ill patients must distinguish these scenarios through clinical correlation and, where possible, documentation of the clinical context before making rejection decisions.
Test-Specific Rejection Criteria Across Laboratory Disciplines
While clotting, hemolysis, insufficient volume, and labeling errors dominate rejection statistics across all disciplines, each major laboratory section applies additional rejection criteria specific to the analytes or organisms it is designed to detect.
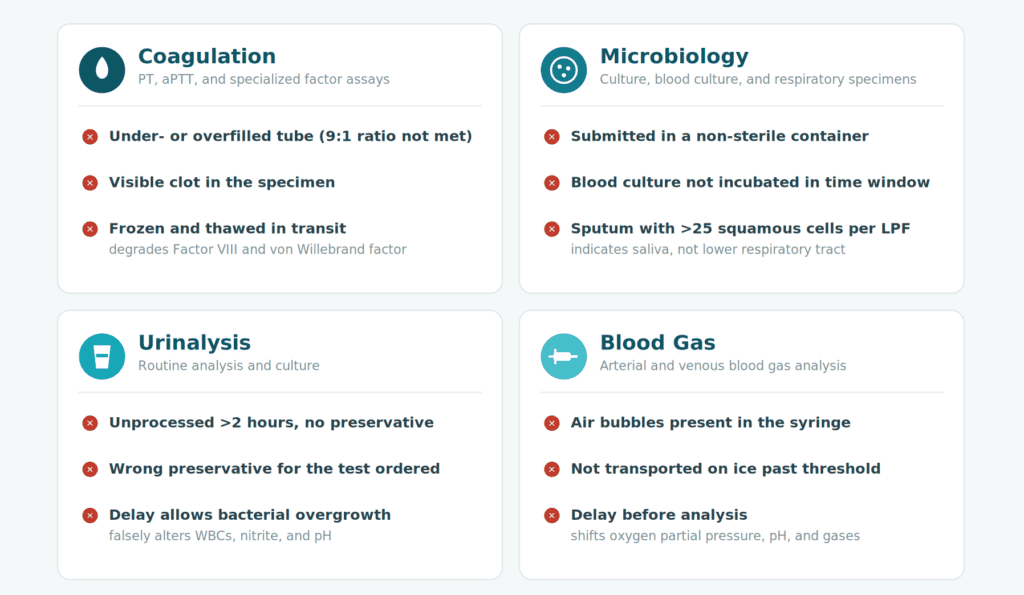
Coagulation studies have the most restrictive volume requirements of any routine blood test discipline, as described above. They also reject samples that have been previously frozen and thawed during transport, because freeze-thaw cycles degrade coagulation factors, particularly Factor VIII and von Willebrand factor, in ways that invalidate both screening and specialized coagulation assays.
Microbiology rejects specimens submitted in non-sterile containers, since contamination from environmental organisms cannot be distinguished from clinically significant pathogens. Blood culture bottles that have not been incubated within the specified time window, aerobic culture specimens incubated beyond the stated stability limit, and respiratory specimens with a Gram stain showing more than 25 squamous epithelial cells per low-power field indicating oral rather than lower respiratory tract origin are all subject to rejection. The squamous epithelial cell threshold exists because a sputum sample contaminated with saliva will culture oral flora rather than the pulmonary pathogen the clinician is trying to identify, producing results that are accurate for what was submitted but clinically useless or actively misleading.
Urinalysis rejects samples that have not been processed within two hours of collection without a preservative, because bacterial overgrowth in unpreserved urine specimens at room temperature produces a falsely elevated white blood cell count, nitrite positivity, and pH changes that can lead to incorrect diagnosis of urinary tract infection. Samples submitted in containers with preservatives designed for 24-hour urine collections are not appropriate for routine culture and sensitivity, and mixing up those containers is a documented source of rejection.
Blood gas analyses reject samples with air bubbles present in the syringe, because exposure to ambient air equilibrates the oxygen partial pressure of the specimen toward atmospheric levels and falsifies the result for the most time-critical parameter being measured. They also reject samples not received on ice when transport time exceeds the threshold for metabolic activity to alter pH and gas concentrations.
The Downstream Impact of Specimen Rejection on Patients and Healthcare Systems
The clinical and operational consequences of specimen rejection are concrete and measurable. An oncology center study published in ScienceDirect found that recollection required by specimen rejection increased turnaround time by an average of 108 minutes per rejected specimen, with total recollection costs across the study period reaching approximately $43,210, averaging $21.90 per rejected sample. A haematology survey found that the median specimen processing delay for inpatients whose samples were rejected was 81 minutes, with delays of 57 minutes for outpatients and 43 minutes for emergency patients. Recollection was required for 84 percent of rejected specimens, meaning that only a small minority could be resolved through dilution, alternate tube, or partial result reporting.
For patients in emergency or critical care settings, an 80-minute delay in a metabolic panel or coagulation result is not merely inconvenient. It delays treatment decisions in time-sensitive situations including acute kidney injury management, sepsis workup, acute coronary syndrome evaluation, and anticoagulation initiation before invasive procedures. Beyond the individual patient level, high institutional rejection rates increase nursing and phlebotomy workload, consume additional laboratory reagents and personnel time on reprocessing, and contribute to clinician frustration and erosion of confidence in laboratory services.
These downstream effects are why institutional specimen rejection rates have become quality indicators tracked by laboratory accreditation programs. CAP quality monitors set benchmarks, and the Joint Commission’s quality improvement literature documents interventions that successfully reduced rejection rates in specific high-acuity units.
Reducing Rejection Rates: What the Evidence Supports
Specimen rejection is predominantly a pre-analytical problem caused by practices that occur before the specimen reaches the laboratory. That means the most effective reduction strategies are also pre-analytical: improving the knowledge and technique of everyone who collects, labels, handles, or transports specimens.
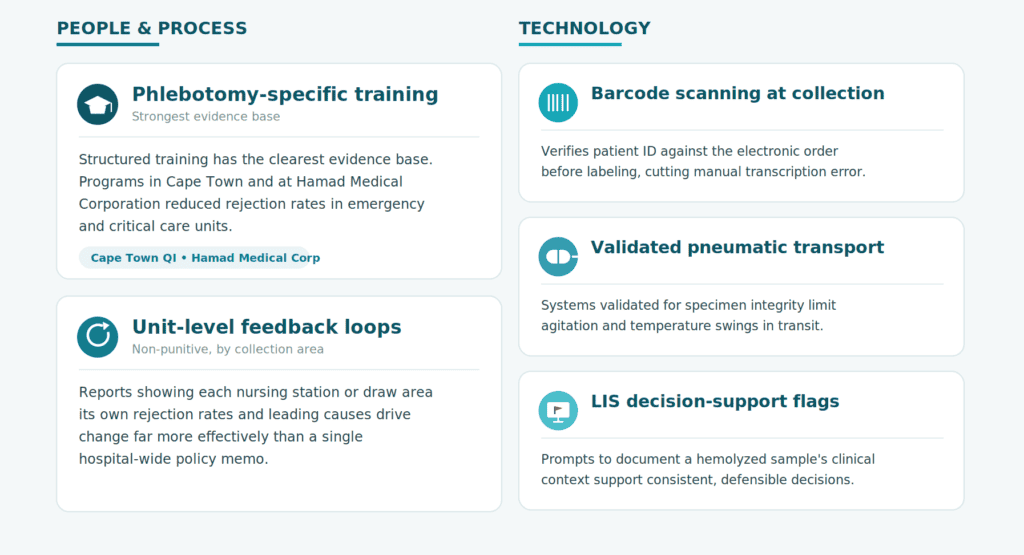
Phlebotomy-specific training has one of the clearest evidence bases for impact. A study in Cape Town examining the effect of phlebotomy training on blood sample rejection among primary healthcare providers found significant reductions in rejection rates following structured training interventions. The Hamad Medical Corporation quality improvement project reported in the Joint Commission Journal on Quality and Patient Safety achieved substantial reductions in ED and coronary ICU rejection rates by implementing targeted phlebotomy education, electronic order standardization, and unit-specific feedback loops providing non-punitive data on rejection reasons and rates by care area.
The specific feedback loop matters. Laboratories that provide unit-level rejection reports, showing nursing stations or collection areas their own rejection rates and the predominant causes, create the accountability and visibility that motivates practice change. Reporting hemolysis rates from a specific ICU back to its nursing manager, with comparison to benchmarks and trend data, is demonstrably more effective than issuing a hospital-wide policy memo.
Technology also plays a role. Barcode scanning at the point of collection that verifies patient identity against the electronic order before the tube is even labeled reduces wrong-patient and mislabeling errors by removing manual transcription from the process entirely. Pneumatic tube transport systems that are properly validated for specimen integrity reduce exposure of samples to mechanical agitation and temperature variation during transit. Electronic flags in the laboratory information system that prompt staff to document the clinical reason for a hemolyzed sample before deciding whether to reject or proceed support more consistent and defensible rejection decisions, particularly in the critical care context where in vivo hemolysis must be distinguished from collection artifact.
Conclusion
Specimen rejection criteria in clinical laboratories exist because a wrong result is more dangerous than no result at all. When a sample is clotted, hemolyzed, mislabeled, underfilled, or transported in a way that degrades the analyte being measured, the laboratory’s obligation to patient safety requires it to stop the process and call for a new specimen rather than report a result it cannot stand behind.
The data consistently show that rejection is concentrated in specific causes, clotted specimens, hemolysis, insufficient volume, and labeling errors, and in specific collection environments, particularly the emergency department and inpatient services where collection conditions are least controlled. The downstream costs of rejection are tangible: delays of over an hour in time-sensitive results, financial costs per recollection, and disruption to clinical workflows. And the interventions that reduce rejection rates are known: structured phlebotomy training, unit-level feedback, point-of-collection technology, and standardized documented criteria applied consistently across all disciplines.
For laboratory medicine to fulfill its role in supporting clinical decisions, the specimen that arrives for analysis must be fit for analysis. Specimen rejection criteria are the mechanism that enforces that standard, and reducing the rate at which rejection becomes necessary is one of the clearest investments a healthcare system can make in diagnostic quality.
Bio-Reach is a non-profit organization committed to advancing laboratory medicine through advocacy, education, and global collaboration. To learn more or get involved, visit bio-reach.org.